Foreign Body Aspiration in Children
What is Foreign Body Aspiration (FBA)?
Foreign body aspiration refers to the inhalation of a foreign object into the airway, typically occurring in children under the age of 5. Children are more prone to foreign body aspiration due to their natural curiosity and tendency to put objects in their mouths. While most incidents involve food, such as peanuts or small pieces of fruit, non-food items like toys, coins, and beads can also be aspirated.
If the foreign body becomes lodged in the airway, it can cause a partial or complete blockage, which can be life-threatening if not treated promptly. Timely diagnosis and intervention are essential to prevent complications such as infections, lung damage, or even death.
Symptoms of Foreign Body Aspiration
The symptoms of foreign body aspiration can vary depending on the size and location of the object, but common signs to watch for include:
- Sudden coughing or choking after swallowing or inhaling an object
- Wheezing or difficulty breathing
- Stridor (a high-pitched sound when breathing)
- Unexplained coughing that lasts for several days
- Respiratory distress or difficulty speaking
- Loss of consciousness (in extreme cases)
If your child exhibits any of these symptoms following an incident where they may have inhaled a foreign object, immediate medical attention is required.
How is Foreign Body Aspiration Diagnosed?
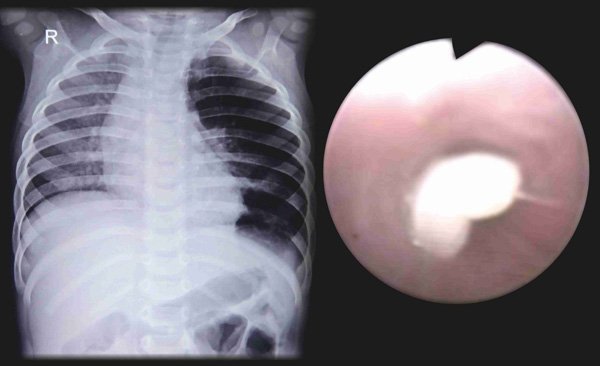
Diagnosing foreign body aspiration involves a thorough clinical evaluation, including a review of the child’s medical history and the circumstances surrounding the choking incident. The physician will perform a physical exam and may request imaging tests such as chest X-rays. Some non-food items (metallic objects like pins, screws, other small metal pieces, etc. ) can be seen in the airway using a conventional radiograph. However, most food, vegetable matter and plastic toys are not radio-opaque, which means they allow X Ray radiation to pass through and hence would not appear on chest X Ray. Collapse or overinflation of a part of the lung on the Chest Xray suggest presence of a foreign body in the lungs. It should be remembered that many children with foreign body aspirations can have normal chest x rays. CT scan of the chest is not very useful to detect a foreign body in the airway. Moreover it exposes the child to significant radiation.
In many cases, the gold standard for diagnosis and treatment is bronchoscopy. A bronchoscopy is a minimally invasive procedure that allows the doctor to look directly into the airways using a flexible tube with a camera. This allows for precise identification of the foreign body and enables the physician to remove it safely.
Complications of foreign body aspiration in children
Large foreign bodies they can be life threatening as they can block the voice box (larynx) or the windpipe (trachea). If small they can lodge in the windpipe or the other smaller airways (bronchi). This can lead to obstruction of a portion of the lung, infections and later can to serious long term damage to the lungs.
Bronchoscopy: The Key to Treating Foreign Body Aspiration
Bronchoscopy plays a crucial role in the treatment of foreign body aspiration. If an object is lodged in the child’s airway, bronchoscopy is often required to visualize and remove the object. During the procedure, a pediatric pulmonologist uses a bronchoscope to examine the airways, locate the foreign body, and carefully extract it without causing further injury.
The procedure is typically performed under minimal sedation to ensure that the child remains still and comfortable during the removal process. Bronchoscopy is a safe and effective method for managing foreign body aspiration and can prevent the need for more invasive surgery.
Prevention of Foreign Body Aspiration
While it’s not always possible to prevent foreign body aspiration, there are steps parents can take to reduce the risk:
- Avoid small objects: Keep small toys, coins, buttons, and other choking hazards out of your child’s reach.
- Supervise eating: Ensure your child sits upright while eating and chews food thoroughly. Avoid foods that are small, hard, or round (e.g., grapes, nuts, popcorn).
- Teach your child: Educate your child about the dangers of putting objects in their mouth.
- Keep hazardous items away: Remove objects like pens, paper clips, and other small household items from areas where children play.
Treatment Options for Foreign Body Aspiration
The treatment for foreign body aspiration depends on the location, size, and nature of the object. If the object is easily visible and accessible, it may be removed through simple measures like coughing or the Heimlich maneuver. However, if the object is lodged deeper in the airways or the child is in distress, bronchoscopy is typically required.
Foreign body aspiration is a serious concern for young children, but with prompt recognition and treatment, it can be managed effectively. If you suspect that your child may have aspirated a foreign object, seek immediate medical attention. With the use of bronchoscopy, many children can recover quickly and avoid long-term complications.
Conclusion
Related Video
Frequently Asked Questions (FAQs)
1. What are the signs that my child has aspirated a foreign object?
Common signs of foreign body aspiration include sudden coughing, choking, wheezing, difficulty breathing, stridor, and unexplained respiratory symptoms that don’t improve. If your child shows any of these signs after a choking incident, seek medical help immediately.
2. How is foreign body aspiration diagnosed in children?
Diagnosis typically involves a physical exam, a review of the child’s symptoms and history, and imaging tests like chest X-rays. In many cases, a bronchoscopy is performed to locate and remove the foreign body.
3. Is bronchoscopy a safe procedure for children?
Yes, bronchoscopy is a safe, minimally invasive procedure commonly performed in children. It is typically done under minimal sedation to ensure the child is comfortable, and complications are rare when performed by an experienced pediatric pulmonologist.
4. Can foreign body aspiration cause long-term damage?
If not treated promptly, foreign body aspiration can lead to complications such as infections, lung damage, or even permanent airway blockage. Early intervention through bronchoscopy can prevent these issues and reduce the risk of long-term damage.
5. How can I prevent foreign body aspiration in my child?
To reduce the risk, avoid small objects that can be swallowed or inhaled, supervise your child while they eat, and teach them to chew food thoroughly. Keeping the environment free from choking hazards and educating your child about the dangers of putting non-food items in their mouth can also help prevent foreign body aspiration.